Nished Rijal.
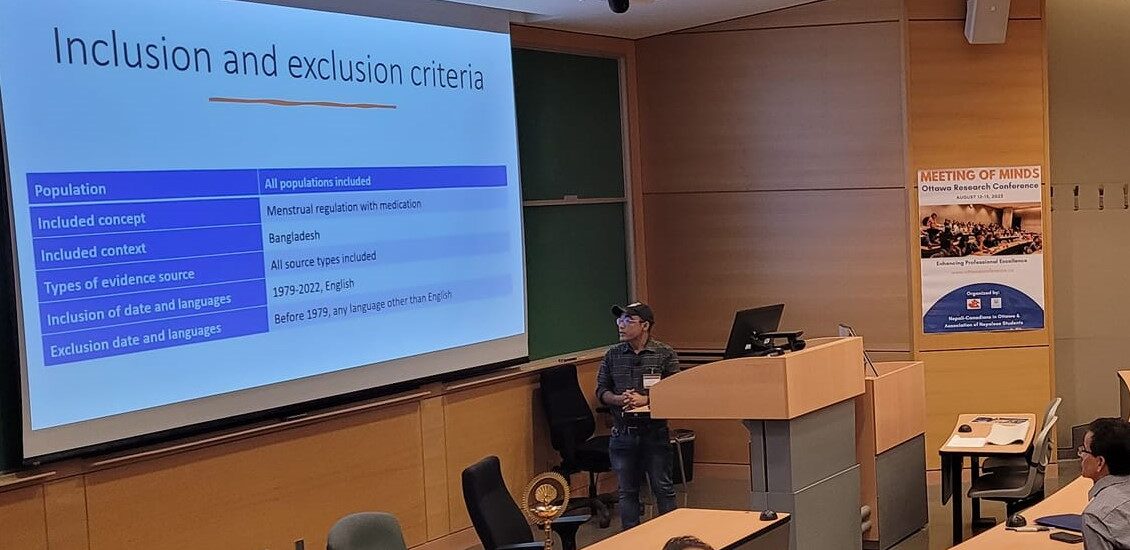
Abortion is a criminal offence in Bangladesh under the Bangladesh Penal Code 1860, permissible only to save a woman’s life. However, Menstrual Regulation (MR), often loosely termed as a provisional to establish non-pregnancy has been part of the national family planning program since 1979. In 2013, Bangladesh introduced Menstrual regulation using medication (MRM) using the mifepristone/misoprostol combination package permitted through 9 weeks of the last menstrual period. Over the last decade, considerable work has been done to increase the use and availability of MRM in Bangladesh. The objective of this scoping review is to gain insight into medication abortion drugs for menstrual regulation available in Bangladesh, with a focus on use and availability in community-based settings and protracted humanitarian settings (Cox’s Bazar). We searched the combination of the keywords in CINAHL, OVID Embase, Medline, and PubMed. We incorporated a grey literature search into this review following the guidelines set forth by CADTH. We charted the data from the sources which were reviewed in full and recorded the following key themes coming from the sources.
We identified 34 sources from the database search and 21 from the grey literature search in the charting table totalling 55 articles. MRM in the context of Bangladesh is still in its infancy and slowly gaining acceptability and popularity among both women and service providers. Only 14% of the government facilities that provide MR services (by Manual Vacuum Aspiration) are providing MRM even though the Bangladeshi pharmaceutical companies are capable of adequately producing the MRM combi-pack locally. Pharmacies and informal providers play a critical role in the availability and use of MRM. First time during any acute emergencies, safe abortion (menstrual regulation) service was introduced and integrated into Minimum Initial Service Package (MISP) for primary health care in the Rohingya refugee camps, though challenges exist. Almost all Bangladeshi women who have used MRM services are either satisfied or highly satisfied although barriers exist on the demand and supply side of the MRM services provision.
Bangladesh is an excellent illustration of how a country recovering from a post-conflict situation and at the same time facing a refugee crisis can still protect women’s right to access menstrual regulation services through a more comprehensive and gendered approach. However, there is an urgent need to improve the supply and increase demand for MRM services in the country, especially in rural areas and urban slums. The government of Bangladesh should ensure continued support and more allocation of resources to ensure MRM commodities, basic and refresher training, monitoring, and supportive supervision. Task-shifting of MRM provision through mid-level providers and mainstreaming of pharmacy provision of MRM services as a harm-reduction approach is remanded. COVID-19 and the Rohingya crisis should be a lesson learned to be more vigilant and establish a contingency plan for similar pandemics or humanitarian crises to ensure uninterrupted provision of sexual and reproductive health services and protect the reproductive rights of Bangladeshi women.
View/Download the presentation from here.
Keywords: Menstrual regulation, menstrual regulation using medication, harm reduction, Bangladesh
Author: Nished Rijal, PhD Candidate
Population Health, Interdisciplinary School of Health Sciences
University of Ottawa, Ottawa, Canada